Breast Reduction
The size of the female breast is influenced by many factors, including heredity, hormonal changes, and body weight. As a result, some women develop problems early in adolescence due to genetic factors, while in others issues appear later in life, during middle age, as a result of hormonal changes.
Regardless of the cause, the problems associated with excessively large breasts are similar: back and neck pain, grooves on the shoulders from bra straps due to weight, rashes and irritation beneath the breasts, difficulty with clothing, and psychological distress.
In some women, there may also be significant asymmetry between the two breasts, with one being much larger than the other.
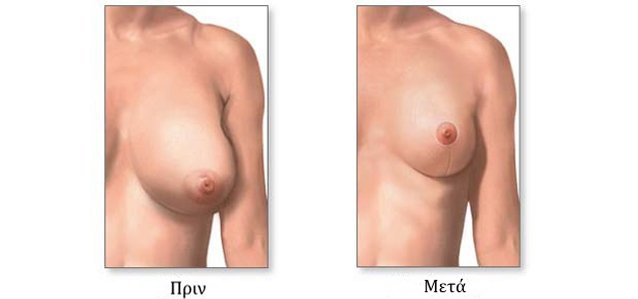
Breast reduction surgery aims to decrease the size of the breasts by removing fat, glandular tissue, and excess skin, making the breasts smaller, lighter, and firmer. At the same time, it can reduce the size of the areola and reposition it to a higher, more youthful position.
How is breast reduction performed?
Each patient’s anatomy and needs are different, so the surgical approach may vary. The procedure is performed under general anesthesia and lasts approximately 2–3 hours.
In most cases, an incision is made around the areola, a second vertical incision extends from the areola down to the breast crease, and a third horizontal incision is made along the inframammary fold, forming an inverted “T” shape. Excess fat, glandular tissue, and skin are removed, the nipple and areola are repositioned higher, and the skin is closed around the breast to create a smaller, firmer, and more youthful contour.
In some cases, the horizontal incision may be short or even unnecessary. Liposuction may also be used as an adjunct in the armpit area to improve breast contour.
In rare cases involving extremely large breasts, the nipple and areola may need to be completely detached and grafted into their new position to ensure adequate blood supply. In such situations, nipple sensation and the ability to breastfeed may be affected.
The sutures are usually internal and absorbable, and two small drains are often placed to prevent fluid accumulation.
What should I expect after surgery?
The procedure lasts about 3 hours, and hospital stay is typically one day. The drains are removed the day after surgery, the dressing is changed, and you may return home.
Postoperatively, you will need to wear a comfortable, wire-free bra (such as a sports bra or nursing bra) for approximately one month. Postoperative pain is usually mild and is managed effectively with simple analgesics such as Lonarid.
Initially, some swelling is expected, which gradually subsides over the next 2–3 months as the breasts settle into their final shape. The scars are initially red and slightly firm, but over time they soften, turn pink, and eventually fade to a lighter color, leaving only minimal marks.
This scar maturation process takes several months but can be accelerated with daily massage.
Sensation around the nipple may initially be reduced but usually returns within a few months.
What complications may occur?
The most common issues involve wound infection, despite preventive antibiotics being routinely administered. If infection occurs, healing may be slightly delayed, but the final result is usually not affected. In cases of very large breasts or in women who smoke, blood supply to the nipple and areola may be compromised. In such situations, complete detachment and repositioning of the nipple-areola complex may be necessary, which can affect sensation and breastfeeding ability. Rarely, minor bleeding may occur and require surgical treatment.
Scarring is not considered a complication, as scars typically mature and become less noticeable over time.
When can I return to normal activities?
From the first or second day after surgery, you may move around freely, although household tasks should be avoided for 1–2 weeks. Return to light work is usually recommended after two weeks, while full return to normal activities is expected after 4–6 weeks.

To book an appointment, please contact us.